
Serum Protein Electrophoresis: Reference Range, Interpretation, Collection and Panels
Various disease states or conditions alter the pattern of proteins in electrophoresis (see Table 1 below).
Table 1. Serum Protein Fractions and Conditions Associated with an Increased or Decreased Level (Open Table in a new window)
Serum Protein Fraction
Increased
Decreased
Albumin
Severe dehydration
Malnutrition, cachexia, liver disease, nephrotic syndrome, protein-losing enteropathies, severe burns
Alpha-1
Inflammatory states, pregnancy
Alpha-1 antitrypsin deficiency
Alpha-2
Inflammatory states, nephrotic syndrome, oral contraceptive use, steroid use, hyperthyroidism
Hemolysis, liver disease
Beta
Hyperlipidemia, iron-deficiency anemia
Hypo-B-lipoproteinemia, malnutrition
Gamma
Polyclonal and Monoclonal Gammopathies
Agammaglobulinemia, hypogammaglobulinemia
Monoclonal gammopathy
A dense narrow band that is composed of a single class of immunoglobulins secreted by an abnormally expanded clone of plasma cells is known as M-protein (paraprotein, monoclonal protein, or M-component).
[3, 4] An M-protein usually presents as a single narrow peak, resembling a “church spire,” in the gamma, beta, or alpha-2 region of the densitometer tracing, or as a dense, discrete band on the agarose gel (see image below).
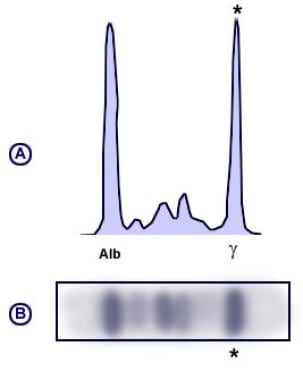
Monoclonal pattern serum protein electrophoresis (SPEP).
View Media Gallery
The monoclonal antibody must be present at a concentration of at least 0.5 g/dL in order to be accurately identified using SPEP. This corresponds to approximately 109 antibody-producing cells.
[5] Plasma cell disorders are typically associated with the presence of an M-protein (see Table 2 below). In addition, an M component may be detected in other lymphoid malignancies like chronic lymphocytic leukemia, any B- or T- cell lymphomas, breast cancer, colon cancer, cirrhosis, sarcoidosis, and other autoimmune disorders.
Conditions associated with a monoclonal increase in the gamma region are as follows:
-
Multiple myeloma
-
Smoldering myeloma
-
Monoclonal gammopathy of undetermined significance (MGUS)
-
Waldenstrom macroglobulinemia
-
Polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes (POEMS syndrome)
-
Solitary plasmacytoma
-
Castleman disease
-
AL amyloidosis
-
Heavy chain deposition disease
-
Light chain deposition disease
Polyclonal gammopathy
Infectious, Inflammatory or various reactive processes may be associated with a broad-based peak or band in the gamma region (Figure 4). This pattern suggests a polyclonal increase in immunoglobulins. Liver disease, autoimmune disease, chronic viral or bacterial infections and various malignancies may cause a polyclonal rise in the gamma fraction (see Table 2 below).
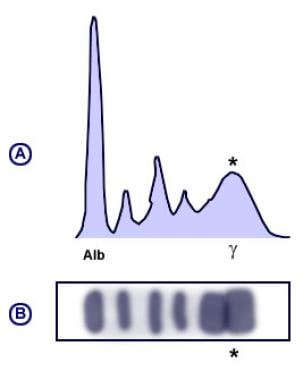
Polyclonal pattern serum protein electrophoresis (SPEP).
View Media Gallery
Table 2. Diseases Associated with a Polyclonal Gammopathy (Open Table in a new window)
Condition
Examples
Liver disease
Cirrhosis, autoimmune or viral hepatitis
Connective tissue diseases
Rheumatoid arthritis, systemic lupus erythematosus, scleroderma, Sjogren syndrome
Infection
Bacterial: osteomyelitis, endocarditis, osteomyelitis
Viral: HIV/AIDS, hepatitis C, Epstein-Barr virus
Hematologic disorders/malignancies
Non-Hodgkin lymphoma, chronic lymphocytic leukemia, thalassemia, sickle cell anemia
Nonhematologic malignancies
Lung, ovarian, gastric malignancies, hepatocellular carcinoma
Considerations
The presence of an M-protein may be missed if the level is too small to be detected using SPEP. In cases where a high suspicion for a clonal plasma cell disorder is high, more sensitive tests such as a serum immunofixation or free light chain assay should be performed. In addition, when either alpha-1 antitrypsin deficiency or immunoglobulin deficiency, specific quantitation is indicated as SPEP is insensitive in these cases.
Therapeutic monoclonal antibodies can interfere with results on SPEP and immunofixation. For example, a study by Scholl et al found that when casirivimab plus imdevimab, used in the treatment of coronavirus disease 2019 (COVID-19), was tested in serum samples, imdevimab produced “sustained assay interference (for at least 6 weeks) that could be misinterpreted as an IgG lambda monoclonal gammopathy.”
[6]





